

Interventional cardiology (also known as invasive cardiology) refers to diagnostic and therapeutic cardiac procedures that can be performed using catheters. Today, interventional cardiology occupies a leading position in the treatment of cardiovascular diseases and is helping to steadily reduce the mortality rate of patients with diseases such as heart attacks, severe cardiac insufficiency or heart valve disease.
Interview with Prof. Dr. Wenaweser
What options does interventional cardiology offer?
Prof. Dr. med. Peter M. Wenaweser – Interventional Cardiology – HerzKlinik Hirslanden
New methods have been developed in interventional cardiology in recent years that have revolutionised treatment options. Depending on the clinical picture, a specific vascular access is selected through which the catheters are inserted.
Interventional cardiological techniques are an important cornerstone in the treatment of cardiovascular diseases and complement advances in rhythmology, the treatment of heart failure, cardiac surgery and medication. Thanks to these advances, it is becoming increasingly possible to offer patients high-quality, minimally invasive therapy.
How is the intervention carried out via the radial artery of the wrist?
Most investigations and interventions on the coronary arteries can be carried out using catheters (2-3 mm in diameter) inserted via this access (see figure a). Balloon dilatation (PTCA, widening of a narrowed coronary artery) is still the most common procedure in interventional cardiology and enables the rapid and safe treatment of coronary heart disease by means of stent implantation (vascular support). Currently, drug-eluting stents (DES) are routinely used as they have a very low re-narrowing rate (restenosis). Newer stent technologies such as absorbable stents (BVS), which dissolve over time, are only being used selectively and still have to prove themselves against the established DES in comparative studies and in everyday clinical practice. The elegant access via the wrist artery enables the patient to get up immediately after the procedure and leave the clinic on the same day. In addition, the risk of bleeding is lower than with access via the inguinal artery.
Intervention via the inguinal artery (femoral artery)?
The inguinal artery (see figure b) is the standard access for complex interventions on the coronary arteries and, thanks to the larger vessel diameter, offers more options for highly specialised interventions. This approach is particularly important for the treatment and diagnosis of valvular heart disease. Minimally invasive aortic valve replacement (TAVI) is a routine procedure at specialised centres and is superior to open heart surgery in selected patients. Detailed preliminary examinations using ultrasound and other imaging procedures (computer tomography) are a prerequisite for successful application. The majority of TAVI procedures can be performed without a general anaesthetic. For the remaining patients, access via the apex of the heart (transapical – see figure d) or introduction of the system via the subclavian artery (see figure c) can be considered. Interventions on the leg, neck or kidney vessels can also be performed via the inguinal artery.
Intervention via the inguinal vein (femoral vein)?
Procedures via the venous access (see figure e) are generally less prone to complications due to the lower pressure compared to the arterial area. It is typically used for blood flow measurements (haemodynamic measurements), tissue samples (heart muscle biopsies) and evaluation of pulmonary pressure. Congenital heart defects (shunt defects) such as atrial septal defect (ASD) or persistent foramen ovale (PFO), an open connection between the right and left atrium, are also closed or treated via this access. Such a connection harbours the risk of overloading the circulation or heart failure as well as thrombotic complications that can lead to a stroke: Small clots that have formed in the leg veins are not intercepted in the pulmonary circulation, but pass directly into the arterial bloodstream and, in the worst case, block a cerebral artery. With so-called umbrella implantation, such defects can be easily repaired – without heart surgery.
Transseptal puncture: Intervention via the cardiac septum?
The venous access is also used to perform a transseptal puncture (puncture of the cardiac septum). This deliberately creates a connection between the right and left atrium, enabling interventions on the mitral valve, the valve between the left atrium and the left ventricle, such as balloon dilation of a narrowed valve or the catheter procedure for a leaky valve (mitral clip). In recent years, the mitral clip procedure has established itself as a good alternative for high-risk patients with severe leakage of the mitral valve. The leak is closed with a clip. Ultrasound technology and fluoroscopy technology must be combined for successful application. The hybrid operating theatre offers the ideal conditions for this. As with TAVI procedures, this also requires a highly specialised team.
In addition, transseptal puncture can also be used to close the left atrial appendage (LAA), which is a niche for clot formation in patients with atrial fibrillation. This newer technique involves the cardiologist closing the left atrial appendage with an implant. This eliminates the main source of embolism and reduces the risk of stroke. In particular, patients who are taking blood-thinning therapy for atrial fibrillation and are prone to bleeding benefit from atrial appendage closure. After closure, long-term therapy with aspirin alone is possible.
Diagram of diagnostic and therapeutic approaches in interventional cardiology:
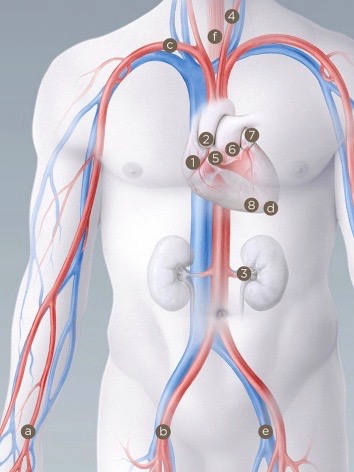
a Wrist artery (radial artery) for
1 Coronary arteries (balloon dilatation / stenting)
b Inguinal artery (femoral artery) for
1 coronary arteries (balloon dilatation / stenting), 2 aortic valve (TAVI), 3 renal artery, 4 carotid artery
c subclavian artery, for 2 aortic valves (TAVI)
d Transapical access, for
2 Aortic valve (TAVI)
inguinal vein (femoral vein), for
5 Cardiac septum / foramen ovale (umbrella device / blood flow measurement / transseptal puncture), 6 Mitral valve (reconstruction / mitral clip), 7 Left atrial appendage (closure) and 8 Cardiac muscle (biopsy)
